| Issue |
Vis Cancer Med
Volume 7, 2026
|
|
|---|---|---|
| Article Number | 2 | |
| Number of page(s) | 6 | |
| DOI | https://doi.org/10.1051/vcm/2026003 | |
| Published online | 20 April 2026 | |
Original Research Article
Oral carcinoma cuniculatum: A rare entity with diagnostic challenges. A series of 5 cases and review of literature
1
Department of Surgical Oncology, Dr. B. Borooah Cancer Institute, Guwahati, Assam, India
2
Department of Oncopathology, Dr. B. Borooah Cancer Institute, Guwahati, Assam, India
3
Department of Head and Neck Oncolog, Dr. B. Borooah Cancer Institute, Guwahati, Assam, India
* Corresponding author: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
1
November
2025
Accepted:
22
February
2026
Abstract
Carcinoma cuniculatum (CC) is an uncommon variant of squamous cell carcinoma (SCC). It is a low-grade tumor with an endophytic and burrowing growth pattern. The lesion initially presents as a condyloma or a hyperkeratinized patch, which eventually ulcerates and features sinuses that discharge keratinous material. To date, CC remains rare, with about 75 reported cases, and it is frequently missed or misdiagnosed. The aim of the present work is to report five cases of CC in the gingivobuccal complex and highlight its main clinicopathological diagnostic features: an exophytic cobblestone surface and a characteristic endophytic burrowing architecture, as well as to differentiate it from other closely similar lesions, including verrucous carcinoma, papillary squamous cell carcinoma, and well-differentiated conventional oral squamous cell carcinoma. An accurate diagnosis of CC requires clinicians’ and pathologists’ awareness of this entity, a thorough understanding of the diagnostic clinical and histopathological evidence, and the ability to differentiate it from similar lesions.
Key words: Oral carcinoma cuniculatum / Rabbit burrows / Verrucous carcinoma
© The Authors, published by EDP Sciences, 2026
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Carcinoma cuniculatum (CC), also known as cuniculate carcinoma, is a rare low- grade carcinoma [1]. Arid et al. reported the first case series of CC on the plantar surface of the foot [2]. CC has been documented in other locations, including the abdominal wall, skin, and genital region [3]. However, the oral cavity was first identified as a site for CC by Flieger and Owinski [4]. Numerous synonyms have been used to describe this entity, including epithelioma cuniculatum, Buschke–Lowenstein tumor, and inverted verrucous carcinoma (VC) [5]. Regarding its unique clinical and pathological aspects, the World Health Organization (WHO) recognized CC of the oral cavity, referred to as oral carcinoma cuniculatum (OCC), as a distinct, well-differentiated subtype of oral squamous cell carcinoma (OSCC) in 2005 and 2017. OCC and VC were also considered different subtypes, although they are often confused [6]. OCC remains a rare entity that presents diagnostic challenges, with approximately 75 cases documented in the literature from 1977 to May 2021 [7]. Herein, we present five OCC cases.
Methodology
Clinical and pathology data for all cases of CC arising in the oral cavity were retrieved from the archives of the Department of Pathology at our tertiary-care oncology institute. Haematoxylin and eosin-stained slides for all cases were collected. Clinical findings and treatment details were recorded from the hospital’s electronic medical records. The recorded demographic and clinical parameters included age, gender, imaging features (computerized tomography, tumor location, and size, type of resection, clinical staging, and treatment administered). The pathology features analyzed included tumor size (pT), histologic type, grade, architectural growth patterns, depth of invasion (DOI), pattern of invasion (POI), lymphovascular invasion (LVI), perineural invasion (PNI), surgical margins, lymph node (LN) status, and pathologic TNM staging as per the AJCC, 8th edition (Figures 1–3; Tables 1 and 2).
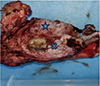 |
Figure 1 Gross image of the tumour showing the ulceroproliferative tumour involving buccal Mucosa (blue star), lower gingivobuccal sulcus (blue cross) and mandible (blue arrow). |
 |
Figure 2 (A) Radiology showing bony erosion of the mandible (marked by red arrows) and (B) gross image of the tumour of the same patient showing the ulceroproliferative tumour involving lower gingivobuccal sulcus (black arrows) and mandible. |
 |
Figure 3 (A) 10× view showing proliferating well differentiated squamous epithelium (black arrow); (B) 10× view showing the burrowing nature (black arrow) of Carcinoma cuniculatum; (C) and (D): 40× view of the well differentiated squamous epithelium with no dysplasia (black arrow). |
Summary of all the five cases.
Discussion
Carcinoma cuniculatum of the oral cavity is a rare variant of SCC as it is under-recognized among both, pathologists and oncologists, even five decades after it was first described in the head and neck region. Sun et al. in their study with 540 cases of SCC [8]. Cases are mostly reported in the sixth and seventh decades with female preponderance [9]. In our study, one case out of five was found in the 4th decade, with a male preponderance, which was also reported in other studies [10, 11].
The most frequently reported sites of origin of oral CC were the alveolus and hard palate [12]; in our study, the buccal mucosa was the most common site. The exact aetiology and causative mechanisms, as suggested by multiple studies, are long- standing (neuropathic) ulcers, trauma, tobacco, alcohol, poor oral hygiene, and human papillomavirus (HPV; types 1–4, 6, 11, and 18), along with tobacco consumption and smoking [8, 12, 13]. All our patients had a history of smoking and tobacco cessation.
The three histologic features that characterise Carcinoma cuniculatum are [14]:
1) a complex architecture with branching sinuses and keratin-filled cysts resembling the eponymous rabbit cuniculus (burrow); 2) broad and bulbous rete pegs; and 3) lack of (or minimal) cytologic atypia. The usual growth pattern of CC is predominantly an endophytic component of well-differentiated squamous cells that forms tortuous, deep sinuses and interconnected, elongated, cavernous cavities filled with abundant keratin, with a variable exophytic component. All our cases showed these distinctive keratin-filled cavities. Owing to the deeply infiltrative growth pattern in CC, these tumours are locally aggressive. Two of our cases showed bone infiltration. Intraepithelial neutrophils and a prominent cuff of lymphocytes, plasma cells, foreign-body giant cells, and microabscesses at the tumour edge are often seen. Perineural invasion and LVI are usually not a feature of oral CC. None of our cases showed LVI and PNI.
The closest differential diagnosis is Verrucous carcinoma (VC), characterised by mostly exophytic growth, formed by well-differentiated squamous cells. Branching and interconnected cyst-like sinuses filled with keratin are absent in VC, which are pathognomic of CC. Nodal metastasis is uncommon in both.
The diagnosis of CC is possible only in resected specimens in which the pathognomic architecture is seen. Lack of atypia and the tumour mostly being infiltrative, the diagnosis in a punch biopsy is often missed.
The primary modality of treatment is surgery with clear margins. RT and CT do not appear to play a significant role in CC. Lymph nodal metastases are reported in 14–24% of cases [15, 16]. Despite being locally aggressive and rare instances of metastases, the prognosis is favourable [17]. Local recurrences have been reported irrespective of free margins in 3–27% [18]. In our study, the minimum follow-up was 1 year, and only one patient showed local recurrence.
Conclusion
Although rare, awareness of OCC among pathologists, oncosurgeons, and oncologists can be helpful in the recognition and better management of these cases. More studies with longer follow-up are necessary to determine the metastatic potential and recurrence.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of interest
The authors declare that they have no conflicts of interest related to this study.
Data availability statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request. The data are not publicly available due to institutional policies and patient confidentiality.
Author contribution statement
M.M contributed to study conception, surgical management, data collection, and manuscript drafting. A.S contributed to histopathological evaluation, manuscript editing, and the article submission process. S.B. contributed to clinical management and review of the manuscript. A.K.D., T.R., R.B., S.A., and L.K. contributed to the analysis, and critical revision of the manuscript. All authors read and approved the final manuscript.
Ethics approval
This study was approved by the Institutional Ethics Committee of Dr B. Borooah Cancer Institute, Guwahati. Given the retrospective nature of the study and use of anonymized patient data, the requirement for informed consent was waived.
References
- Barnes L, Universitäts Spital Zürich, Departement Pathologie, International Academy of Pathology, World Health Organization, International Agency for Research on Cancer, et al. Pathology and genetics of head and neck tumours: tumours of the oral cavity and oropharynx. Lyon: International Agency for Research on Cancer (IARC) Press; 2005. p. 163–175. [Google Scholar]
- Aird I, Johnson HD, Lennox B, Stansfeld AG. Epithelioma cuniculatum: a variety of squamous carcinoma peculiar to the foot. Br J. 1954;42(173):245–250. [Google Scholar]
- Kao GF, Graham JH, Helwig EB. Carcinoma cuniculatum (verrucous carcinoma of the skin): a clinicopathologic study of 46 cases with ultrastructural observations. Cancer. 1982;49(11):2395–2403 [Google Scholar]
- Flieger S, Owiński T. Epithelioma cuniculatum an unusual form of mouth and jaw neoplasm. Czas Stomatol. 1977;30(5):395–401. [Google Scholar]
- Barreto JE, Velazquez EF, Ayala E, Torres J, Cubilla AL. Carcinoma cuniculatum: a distinctive variant of penile squamous cell carcinoma - report of 7 cases. Am J Surg Pathol. 2007;31(1):71–75. [Google Scholar]
- Yadav S, Bal M, Rane S, Mittal N, Janu A, Patil A. Carcinoma cuniculatum of the oral cavity: a series of 6 cases and review of literature. Head Neck Pathol. 2022;16(1):213–223. [Google Scholar]
- Farag AF, Abou-Alnour DA, Abu-Taleb NS. Oral carcinoma cuniculatum, an unacquainted variant of oral squamous cell carcinoma: a systematic review. Imaging Sci Dent. 2018;48(4):233–244. [Google Scholar]
- Sun Y, Kma K, Burkhardt A, Yamamoto H. Clinicopatho logical evaluation of carcinoma cuniculatum: a variant of oral squamous cell carcinoma. J Oral Pathol Med. 2012;41:303–308. [Google Scholar]
- Thavaraj S, Cobb A, Kalavrezos N, Beale T, Walker DM, Jay A. Carcinoma cuniculatum arising in the tongue. Head Neck Pathol. 2012;6:130–134. [Google Scholar]
- Flieger S, Owiński T. Epithelioma cuniculatum an unusual form of mouth and jaw neoplasm. Czas Stomatol. 1977;30:395–401. [Google Scholar]
- Delahaye JF, Janser JC, Rodier JF, Auge B. Le carcinome cuniculatum. 6 observations et revue de la littérature. J Chir. 1994;131:73–78. [Google Scholar]
- Thibouw F, Anna H, Levasseur J, Mondoloni C, Aubriot-Lorton MH, Zwetyenga N. Carcinoma cuniculatum of the lip: a case report. J Stomatol Oral Maxillofac Surg. 2018;119: 224–228. [Google Scholar]
- Sivapathasundharam B, Kavitha B, Padmapriya VM. Carcinoma Cuniculatum of the alveolar mucosa: a rare variant of squamous cell carcinoma. Head Neck Pathol. 2019;13:652–655. [Google Scholar]
- Padilla RJ, Murrah VA. Carcinoma cuniculatum of the oral mucosa: a potentially underdiagnosed entity in the absence of clinical correlation. Oral Surg Oral Med Oral Pathol Oral Radiol. 2014;118:684–693. [Google Scholar]
- Kruse AL, Graetz KW. Carcinoma cuniculatum: a rare entity in the oral cavity. J Craniofac Surg. 2009;20:1270–1272. [Google Scholar]
- Shapiro MC, Wong B, O’Brien MJ, Salama A. Mandibular destruction secondary to invasion by carcinoma cuniculatum. J Oral Maxillofac Surg. 2015;73:2343–2351. [Google Scholar]
- Pons Y, Kerrary S, Cox A, Guerre A, Bertolus C, Gruffaz F, Capron F, Goudot P, Ruhin-Poncet B. Mandibular cuniculatum carcinoma: apropos of 3 cases and literature review. Head Neck. 2012;34:291–295. [Google Scholar]
- Shapiro MC, Wong B, O’Brien MJ, Salama A. Mandibular destruction secondary to invasion by carcinoma cuniculatum. J Oral Maxillofac Surg. 2015;73:2343–2351. [Google Scholar]
Cite this article as: Malhotra M, Suhana A, Basuroy S, Das AK, Rahman T, Bezbaruah R, Ahmed S, Kakoti L. Oral carcinoma cuniculatum: A rare entity with diagnostic challenges. A series of 5 cases and review of literature. Visualized Cancer Medicine. 2026; 7, 2. https://doi.org/10.1051/vcm/2026003
All Tables
All Figures
|
Figure 1 Gross image of the tumour showing the ulceroproliferative tumour involving buccal Mucosa (blue star), lower gingivobuccal sulcus (blue cross) and mandible (blue arrow). |
| In the text | |
|
Figure 2 (A) Radiology showing bony erosion of the mandible (marked by red arrows) and (B) gross image of the tumour of the same patient showing the ulceroproliferative tumour involving lower gingivobuccal sulcus (black arrows) and mandible. |
| In the text | |
|
Figure 3 (A) 10× view showing proliferating well differentiated squamous epithelium (black arrow); (B) 10× view showing the burrowing nature (black arrow) of Carcinoma cuniculatum; (C) and (D): 40× view of the well differentiated squamous epithelium with no dysplasia (black arrow). |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.